



7 yr old presents with fever cough and sorethroat of 3 days duration . His grand father tested positive for corona by antigen test
Is he likely to be positive?
If he is negative when should he be tested again ?
what is corona virus?
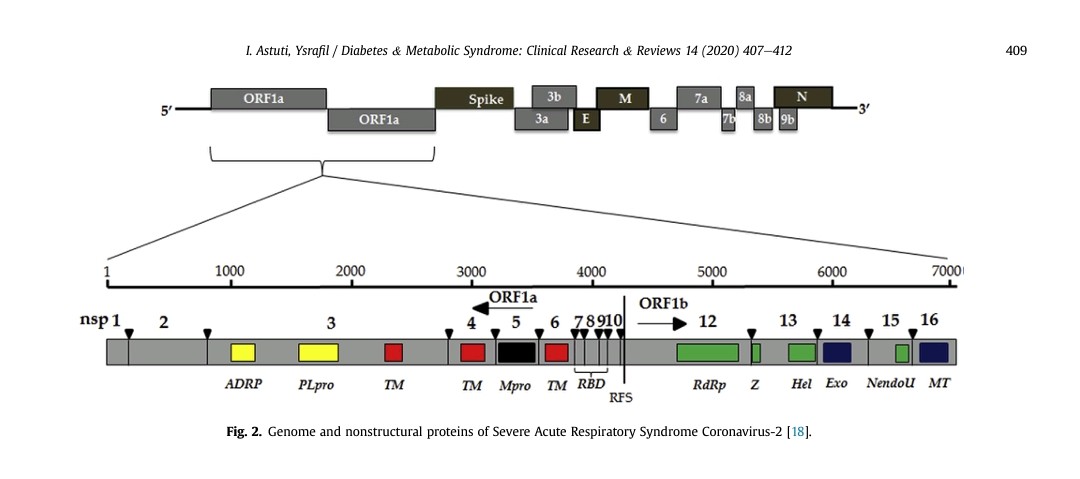
Coronaviruses are medium to large enveloped RNA viruses. It has a characteristic widely spaced, petal shaped surface projections, making the virus look like solar corona. The viruses are heat labile and also vulnerable to lipid solvents and alkaline pH.
Coronavirus is positive sense, single stranded RNA of 30 kilobases in length. (Single stranded RNA viruses are classified as positive or negative depending on the sense or polarity of the RNA. The positive-sense viral RNA genome can serve as messenger RNA and can be translated into protein in the host cell)

What is sars cov 2?
SARS-CoV-2 The current pandemic caused by SARS -CoV-2 which emerged initially in Wuhan, China is rapidly spreading and so far has affected 216 countries with 3,00,441 deaths (as on May 16, 2020).6 It was initially named as 2019 novel coronavirus because of the incomplete match between the genomes of this and other (previously known) coronaviruses.7 This pathogen was later renamed as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by the Coronavirus Study Group and the disease was named coronavirus disease 2019 (COVID-19) by the WHO.8 The incubation period of SARS-CoV-2 is estimated to be between 1 and 14 days, with a median of 5 to 7 days.
How is it transmitted?
Infections occur through respiratory route. Aerosols are generated during cough, sneeze or even while talking. It consists of saliva and nasopharyngeal secretions that are contaminated with infectious agents. The droplets can be propelled for some distance depending upon their size and force of expulsion. The expelled droplets can land directly on the conjunctiva, oro-respiratory passage or skin of a close contact.
Small droplets less than 5μm can travel rapidly and to some distance depending upon the external environment. During dry season with less humidity, the moisture in these particles evaporate to produce droplet nuclei which are light and can remain airborne for a long time. Respiratory droplets can also contaminate inanimate objects.
Touching these objects with contaminated fingers following cough or sneeze can transmit infection. In healthy children, HCoV replicates only in the upper respiratory tract. The incubation period is generally 2 days and the infection lasts for about a week. Infection in immune-compromised children may be severe.
What are the manifestations of covid?
Upper respiratory tract infection: HCoV often presents like an undifferentiated acute respiratory tract infection. Rhinorrhea, sore throat, cough, malaise, headache and fever are the usual features.
Lower respiratory tract infection: HCoV is the third most common etiology of viral pneumonia and bronchiolitis after respiratory syncytial virus (RSV) and parainfluenza virus. It may also precipitate acute asthma. HCoV may affect neonates and clinically present with apnea, hypoxia and bradycardia.
Enteric infection: There are reports of nursery outbreaks of severe diarrhea and necrotizing enterocolitis (NEC) related to HCoV.1
Neurologic diseases: HCoV is linked to neurological diseases like acute disseminated encephalomyelitis (ADEM), multiple sclerosis and polyradiculitis.
What is Basic reproductive number – R0?
To calculate the degree of contagiousness or transmissibility of the coronavirus (infectivity), epidemiologists use different mathematical formulae to calculate the infectivity index. For this purpose, “basic reproductive number” R0(pronounced as R naught or R zero) is used. It is defined as the average number of new infections generated by an infectious person in a totally naïve (uninfected) population.19
It determines the herd immunity threshold and therefore the immunization coverage required to eliminate the disease.
If R0 is >1, the number of people infected is likely to increase and if R0 is <1, transmission is likely to die out.
What are the stages of covid 19?

What are the clinical types?

When will you suspect covid?
• Any acute illness with no other explainable cause
• Fever with or without associated respiratory/ gastrointestinal manifestations
• Runny nose, sore throat, cough, loss of sense of taste or smell
• Myalgia, fatigue
• Abdominal pain, diarrhea and vomiting • Irritability, drowsiness, seizures, stroke • Breathlessness, tachypnea, hypoxia
• Manifestations of pediatric multi system inflammatory syndrome including fever, conjunctivitis, rash, hypotension
How to dx?
RT PCR
ANTIGEN TEST
Molecular tests (Nucleic acid amplification tests/ NAAT)
NAAT tests conducted on respiratory secretions are currently the gold standard for diagnosing COVID-19. The most common NAAT assays in commercial use are the RT-PCR tests. These tests have two targets. The first screening gene is the generic coronavirus gene coding for either the spike protein (S), nucleocapsid protein (N), envelope protein (E) or membrane protein (M). The second target is the gene specific to COVID-19 which could be the gene coding for RNA dependent RNA polymerase or spike protein (S) or the open reading frame, ORF 1 or 2. Hence, the sensitivity of kits may vary depending on the target genes used.
Collection of samples
The molecular test is performed on respiratory secretions which can be collected from the upper respiratory (nasal swab, oropharyngeal swab, nasopharyngeal swab) or lower respiratory (sputum, endotracheal aspirate, bronchoalveolar lavage) tracts.

What is the latest advisory by ICMR for testing?

In Hospital Settings:
Choice of Test (in order of priority):
i. RT-PCR or TrueNat or CBNAAT
ii. Rapid Antigen Test (RAT) 9.
All patients of Severe Acute Respiratory Infection (SARI). 10. All symptomatic (ILI symptoms) patients presenting in a healthcare setting. 11.
Asymptomatic high-risk patients who are hospitalized or seeking immediate hospitalization such as immunocompromised individuals, patients diagnosed with malignant disease, transplant patients, patients with chronic co-morbidities, elderly ≥ 65 years. 12.
Asymptomatic patients undergoing surgical / non-surgical invasive procedures (not to be tested more than once a week during hospital stay). 13
. All pregnant women in/near labor who are hospitalized for delivery. Points to be noted: No emergency procedure (including deliveries) should be delayed for lack of test. However, sample can be sent for testing if indicated as above (1-13), simultaneously. Pregnant women should not be referred for a lack of testing facility. All arrangements should be made to collect and transfer samples to testing facilities.
Mothers who test positive for COVID-19 should be advised to wear a mask and undertake frequent handwashing while handling their baby for 14 days. They should also be advised on breast cleaning before feeding the neonate. These measures are likely to reduce transmission of COVID-19 to their babies.
14. All symptomatic neonates presenting with acute respiratory / sepsis like illness. (Features suggestive of acute respiratory illness in a neonate are respiratory distress or apnea with or without cough, with or without fever. Neonates may also manifest with only non-respiratory symptoms like fever, lethargy, poor feeding, seizures or diarrhea).
15. Patients presenting with atypical manifestations [stroke, encephalitis, hemoptysis, pulmonary embolism, acute coronary symptoms, Guillain Barre syndrome, Multiple Organ Dysfunction Syndrome, progressive gastrointestinal symptoms, Kawasaki Disease (in pediatric age group)] based on the discretion of the treating physician.
What is the management?
Clinical categorisation for planning therapy All children with suspected COVID-19 infection should be categorized into three categories.
Category A
patients (mildly symptomatic patients) These patients can be sent home or to COVID-19 care centres with supportive care. Avoid using non-steroidal anti-inflammatory drugs other than paracetamol. Advice regarding prevention and treatment of dehydration with ORS and appropriate use of other home available fluids in case of diarrhea and vomiting. Patients should be clearly instructed about danger signs and the occurrence of any new symptom or worsening of existing symptom warrants review. These patients should be reviewed every 24-48 hours.
Telemedicine facilities may be used for reviewing mildly symptomatic patients. Patients may be offered zinc 2mg/kg/day, (maximum 20 mg) especially in the presence of diarrhea. All category A patients with a history of contact with a confirmed case of COVID 19 should be tested for COVID 19 with a nasopharyngeal swab.
Category B
patients (moderate symptoms/ patient with comorbidities)
Admission: These patients may be preferably admitted in isolation wards and nasopharyngeal swabs sent for confirmation of disease. Children with comorbidities also should be admitted in isolation wards. If the health care system is overburdened, those without comorbidities and danger signs can be admitted at COVID-19 care centres or advised to self-quarantine at home with follow up and low threshold for admission in case of worsening of symptoms.
Treatment: They may be started on oseltamivir 3mg/kg/ dose BD if they fulfil the criteria for treatment of Influenza like illness(ILI). WHO clinical case definition “An acute respiratory illness with a measured temperature of > 38°C and cough, with onset within the past 10 days”. Antibiotics as per clinician’s discretion to cover community-acquired pneumonia including atypical pneumonia may be offered. Once swab report is available and the diagnosis confirmed, oseltamivir might be stopped and the patient started on hydroxychloroquine 6.5mg/kg/dose BD on day one followed by 3.25mg/kg/dose BD for four more days along with zinc 2mg/kg/day.7
Category C
patients (severe and critical disease) Category C patients require admission and treatment in high dependency units or ICU’s according to severity of illness.
Admission in ward
• Presence of tachypnea (respiratory rate: <2 months >60/ minute; 2-11 months >50/minute; 1-5 years >40/ minute) without lower chest indrawing or danger signs like lethargy, altered sensorium, inability to feed, convulsion, etc
. • Children with high risk for severe disease with mild symptoms: children with congenital or acquired heart disease, chronic lung, liver, kidney or neurological disease, children on immunosuppressive drugs , congenital or acquired immunodeficiency
• SpO2 90 – 94% without retractions and danger signs. Admission in high dependency unit (HDU)
• SpO2 less than 94% with <2 site retractions • Children with comorbidities with a saturation of less than 94% or tachypnea
. • SpO2 < 90% without increased work of breathing. • Children with tachypnea with lower chest in drawing/ grunt.
Presence of danger signs like inability to feed, altered sensorium, seizure etc. without evidence of shock or other organ involvement (these children may need transfer to PICU early for close monitoring if symptoms persist).
Admission in PICU
• Moderate to severe ARDS ( PaO2/FiO2 (P/F) ratio less than 200 / oxygenation index (OI) < 8 / Oxygen saturation index as measured by FiO2 x mean airway pressure)/SpO2 values (OSI) < 7.5 while on CPAP of minimum 5 cm
• SpO2 < 94% with increased work of breathing (> 2 site retraction/ paradoxical breathing / see saw breathing / head bobbing etc.)
• Suspecting atypical presentation of COVID, i.e., Kawasaki disease (KD) like illness, multisystem inflammatory disorder etc.,
• Shock • Multi-organ dysfunction • Need for mechanical ventilation
• Transfer from ward or HDU for close monitoring / mechanical ventilation
What are the management measures?
Management of admitted patients General measures
• Symptomatic treatment: Avoid giving NSAIDs other than paracetamol for fever. Provide oral bronchodilators or MDI with spacer and mask for children with wheeze.
• Antibiotics and antivirals may be given as per clinicians discretion to cover community-acquired pneumonia, including atypical infections and influenza.
• Ensure euvolemia and advice adequate fluid and feed intake. Monitoring • Vital signs – HR, RR, SpO2, BP • Work of breathing (retractions, use of accessory muscles, grunting, head bobbing, air hunger, large tidal volume breaths)
• Oxygen requirement Laboratory investigations Routine investigations: CBC with differential count and ESR, RFT, LFT, coagulation profile, urine routine and send these in all admitted patients. Unlike adult patients with COVID-19, there have been no consistent leukocyte abnormalities reported in pediatric patients. Only 3.5% of pediatric cases showed lymphopenia.
1 Chest X-ray may show patchy infiltrates consistent with viral pneumonia and chest CT scans may show nodular ground-glass opacities.
Biomarkers in sick children :
CRP, LDH, D-dimer, CPK, ferritin, troponin I, elevated transaminases , prothrombin time, NT-ProBNP, BUN, creatinine.
Send these in patients with severe or critical disease admitted in HDU or PICU and those with worsening respiratory status.
Complications
COVID-19 infection primarily causes upper respiratory infection followed by pneumonitis of varying severity. Some patients progress to develop hyperinflammatory syndrome due to cytokine storm clinically presenting with features of KD,
cytokine release syndrome or infection associated HLH often leading to multi-organ failure.
Pointers towards hyperinflammatory syndrome include
1. Persistent high fever or reappearance of fever.
2. Rising CRP especially more than 100- 200 mg/L
3. Doubling of ferritin in 24 hours or very high ferritin levels (> 2000 – 10,000mcg/L)
4. Falling counts
5. Rising or falling ESR 6. Rising CPK, LDH
7. New-onset shock especially with elevated trop I ( also rule out Kawasaki disease with shock syndrome)
DISCLAIMER
drugs like remdesivir,chloroquine ,osetamavir ,flavipiravir have debatable efficacy
MISC is increasing recognized in children

How to mmunize during g covid?

 Superintendent, ICH.
Superintendent, ICH.